Roux‑en‑Y Gastric Bypass (RYGB) is a benchmark bariatric procedure that reduces stomach volume and reroutes food to alter absorption and gut hormones, producing substantial and durable weight loss.
Gastric Bypass
The Procedure (Key Steps)
- You will be under general anaesthesia, which usually lasts for 2 to 4 hours.
- A small incision will be made, and a laparoscope (a keyhole camera) will be used to access your stomach.
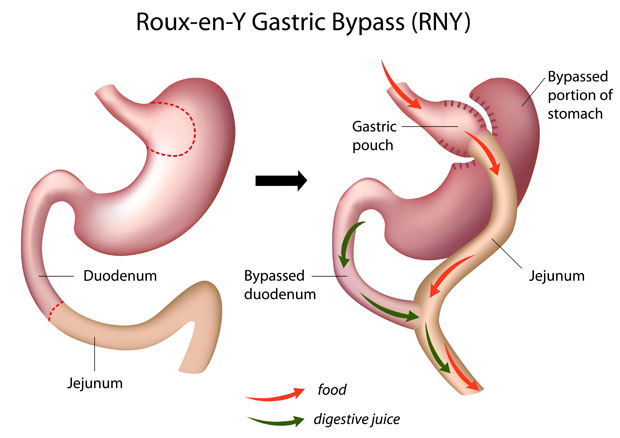
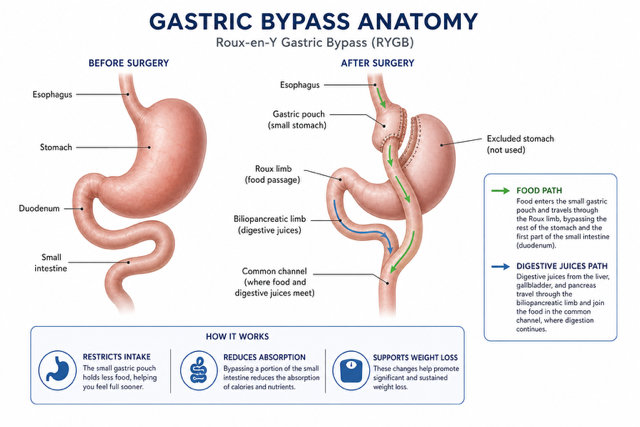
- A gastric pouch, about 30 ml in size, will be created using stapling devices, which will separate it from the rest of your stomach.
- The small intestine will be carefully measured and divided into the right lengths to create new pathways. This process involves making two joints: one between the new stomach and the bowel, and another between the loops of the bowel. These joints are essential because they allow food to enter the intestinal tract and for the stomach acids and digestive enzymes from the bypassed stomach and the first part of the small intestine to mix with the food.
- A dye test (methylene blue test) will be performed using a small tube to check for any leaks.
- Once the test is complete, the instruments will be removed, your abdominal cavity will be deflated, and the cuts will be closed with absorbable stitches.
Expected Outcomes
We anticipate a total weight loss of 35-40% within the first two years. For example, a patient weighing 150 kg is expected to be approximately 95 kg (a loss of 55 kg or 9 stone) in two years.
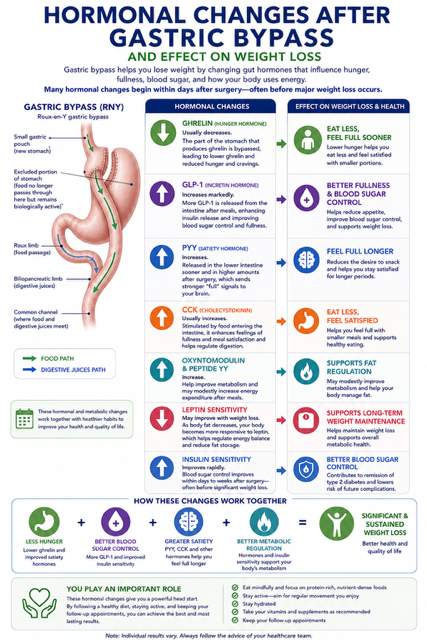
This is accompanied by a significant metabolic impact with frequent remission or improvement of type 2 diabetes, hypertension and dyslipidaemia.
Risks and Complications
- Mortality ≈0.09–0.15%; early complication rate ≈5.9–6.8%.
- Early complication rate ≈5.9–6.8%.
- General complications: pain, bleeding, infection, unsightly scarring, and blood clots.
- Keyhole complications:
– Surgical emphysema: A crackling sensation in your skin caused by trapped gas. It’s usually not serious.
– Incisional hernia: A bulge near a cut caused by deep muscle layers failing to heal. It’s a risk of 1 in 100.
– Damage to other structures: Less than 3 in 1000 risk, especially if you’ve had previous operations. Your surgeon will discuss this with you.
– Conversion to open surgery: A risk of 1 in 100.
Gastric bypass-specific:
- Anastomotic stenosis (~2%)
- Staple-line/anastomotic bleeding (~2%)
- Anastomotic leak (≈1–2%).
- Internal hernia/obstruction (~1%)
- Dumping syndrome
- Gallstones
- Suboptimal weight loss: A risk of 1 in 20
- Nutritional deficiencies: B12, thiamine (B1), iron, calcium, vitamin D, copper, zinc, selenium, vitamin A
Why Mr. Spyros Panagiotopoulos?
Mr. Panagiotopoulos is highly experienced in RYGB and advanced variations (OAGB/SADI‑S/SASI‑S). He prioritises meticulous technique, careful patient selection and rigorous long‑term aftercare.