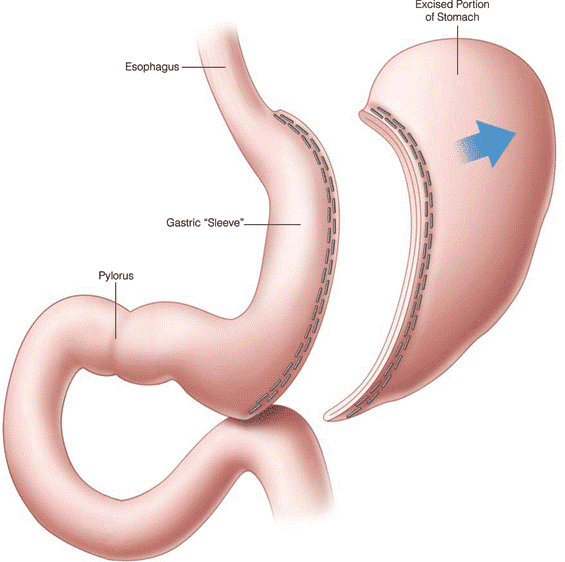
Sleeve gastrectomy removes approximately 80% of the stomach to create a slim, tube‑like pouch. It limits intake and favourably alters gut hormones governing appetite, satiety and glycaemic control.
Sleeve Gastrectomy
The Procedure (Keyhole Surgery)
- General anaesthesia; 1–3 hours typical duration.
- Laparoscopic (keyhole) access with small ports; stomach stapled, divided and resected stomach removed; staple line tested for leaks and reinforced with sutures.
- The staple line will be reinforced with sutures and a test using dye (methylene blue test) will be done using a small tube to verify that there are no leaks.
- At the end the instruments will be removed, deflating your abdominal cavity and the cuts will be closed with absorbable stitches.

How It Works
What happens to your anatomy
Sleeve gastrectomy is simpler than gastric bypass — there’s no rerouting of the intestines. Instead:
- Most of the stomach is removed – Surgeons remove a large portion of the stomach (roughly 75-80%), leaving behind a narrow tube or “sleeve” shape.
- The new stomach is much smaller – This sleeve holds far less food than your original stomach, so you feel full after much smaller meals.
Everything else stays connected – Unlike bypass, food still travels through the same path — stomach, then duodenum, then the rest of the small intestine, in the normal order.

Why you feel less hungry — and full sooner
The key mechanism here is the removal of the part of the stomach that produces most of your body’s ghrelin (the hunger hormone). With less ghrelin, hunger and cravings drop significantly, often within days.
On top of that:
- GLP-1 and PYY (fullness hormones) increase
The stomach after sleeve empties more quickly than before surgery, allowing food to reach the small intestine sooner. This stimulates the release of GLP-1 and PYY, hormones that help you feel full earlier and remain satisfied for longer.
- Insulin sensitivity improves
Insulin sensitivity often improves within days to weeks after surgery, helping improve blood sugar control and contributing to remission or improvement of type 2 diabetes in many patients.
- Leptin sensitivity may improve
As weight loss occurs, the body’s response to leptin — a hormone involved in energy balance and fat storage — may improve, helping support long-term weight regulation.

Expected Outcomes
After sleeve gastrectomy, most patients can expect to lose approximately 25–30% of their total body weight within the first 18–24 months after surgery.
Example
A patient weighing 150 kg before surgery may be expected to reach approximately 105–112 kg within 18-25 months after surgery.
Reaching 105 kg would represent a weight loss of 45 kg (approximately 7 stone).
Health Benefits
Weight loss after sleeve gastrectomy is often accompanied by significant improvements in obesity-related health conditions, including:
- Type 2 diabetes
- High blood pressure (hypertension)
- Abnormal cholesterol or blood fat levels (dyslipidaemia)
- Obstructive sleep apnoea
- Joint pain and mobility problems
- Fatty liver disease
Important Note
Individual results vary. Your own outcomes will depend on factors such as your starting weight, medical conditions, eating habits, physical activity, and long-term follow-up. Your bariatric team can help you understand what outcomes are realistic for you.
Risks and Complications
- Mortality: ≈0.05–0.09%.
- Early (<30 days) complications: ≈3.0–4.8%.
- General complications: pain, bleeding, infection, unsightly scarring, and blood clots.
- Keyhole complications:
– Surgical emphysema: A crackling sensation in your skin caused by trapped gas. It’s usually not serious.
– Incisional hernia: A bulge near a cut caused by deep muscle layers failing to heal. It’s a risk of 1 in 100.
– Damage to other structures: Less than 3 in 1000 risk, especially if you’ve had previous operations. Your surgeon will discuss this with you.
– Conversion to open surgery: A risk of 1 in 100.
- Sleeve‑specific:
– Staple line bleeding: A risk of 1 in 100.
– Staple line leak: A risk of 2 in 100, a serious complication that often requires long-term nutrition support and possibly another operation.
– Sleeve narrowing: A risk of less than 1 in 100.
– Acid reflux: A risk of 5 to 12 in 100.
– Suboptimal weight loss: A risk of 1 in 20.
- Nutritional issues: iron, vitamin D, folate, B1 and B12 deficiencies—prevented with routine supplementation and monitoring.
Why Mr. Spyros Panagiotopoulos?
As an experienced minimally invasive surgeon, Mr. Panagiotopoulos performs sleeve gastrectomy with a focus on safety, precision technique and structured follow‑up to secure lasting outcomes.